Military Flight Physical — What to Expect and How to Prepare
Military flight physicals have gotten complicated with all the misinformation flying around online. As someone who spent months embedded with pilots and aviation medicine specialists watching these evaluations unfold in real time, I learned everything there is to know about what actually happens — and more importantly, what actually trips people up. The single biggest mistake I kept seeing? Applicants showing up completely blind to what the day looks like. So here’s the full picture, across all branches, with the preparation steps that genuinely move the needle.
What the Flight Physical Tests
But what is a military flight physical? In essence, it’s a multi-hour, multi-station medical evaluation designed to catch disqualifying conditions before the military sinks hundreds of thousands of dollars into your training. But it’s much more than that — it’s also your first real test of whether you can prepare for something high-stakes without cutting corners. Plan to be there most of the day. Seriously.
The Core Battery of Tests
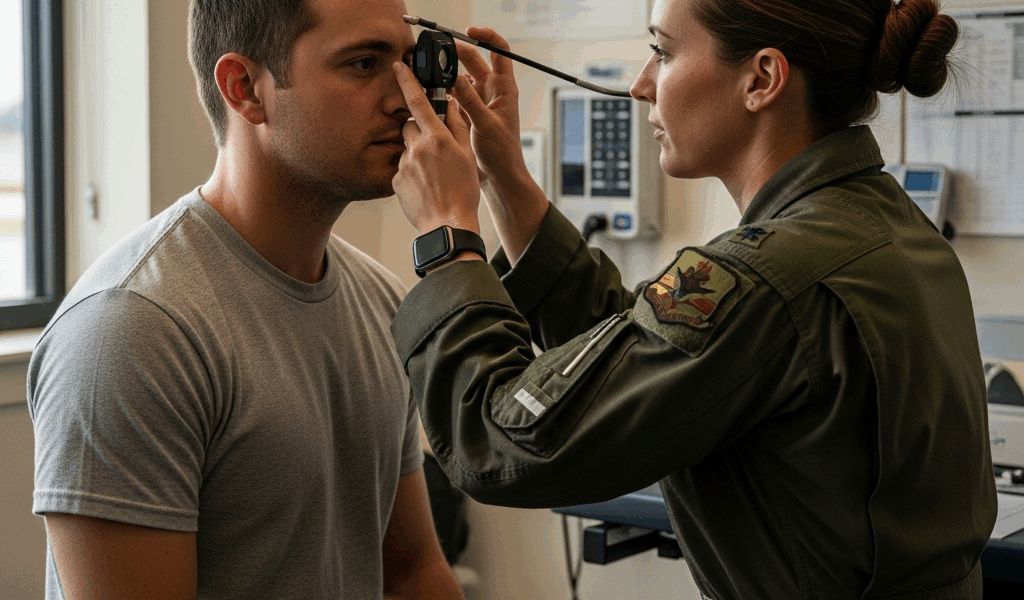
Every branch runs you through a common core. Vision testing comes first — and it’s the most involved station by a wide margin. You’ll do a standard Snellen chart for distance acuity, near vision testing, depth perception usually measured with a Howard-Dolman apparatus, and peripheral vision screening. Then comes color vision. The Pseudoisochromatic Plate (PIP) test is standard, but many facilities now offer the Farnsworth Lantern (FALANT) or the Cone Contrast Test (CCT) as an alternative path if you initially stumble on the plates.
The ophthalmology portion deserves its own paragraph. This is not an optometrist doing a quick refraction. A flight surgeon or ophthalmologist will dilate your pupils and conduct a full slit-lamp examination — corneas, lens, retina, optic nerve, the works. This takes time. The dilation leaves your vision blurred for two to four hours afterward. Do not drive yourself to this appointment. I watched a candidate at Wright-Patterson make exactly that mistake, and we sat in the parking lot for three hours waiting for his eyes to cooperate enough to get him home safely. Don’t make my mistake — or his.
Hearing gets tested through pure-tone audiometry across multiple frequencies. The military cares especially about 500 Hz, 1000 Hz, 2000 Hz, and 3000 Hz — the frequencies that matter for cockpit communication. You’ll sit in a soundproof booth, usually a Tracor or similar audiometric chamber, pressing a button when you hear tones. Straightforward. It still catches a surprising number of people who spent years at loud concerts or shooting ranges without ear protection.
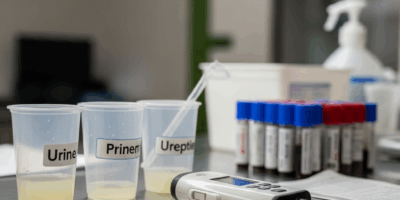
Blood work requires a 12-hour fast before your appointment. They’re pulling a complete metabolic panel, CBC, lipid panel, and glucose. Some facilities add thyroid function. The glucose test specifically is why the fast matters — showing up after a bagel and coffee will get your appointment rescheduled on the spot. Urinalysis is also required, screening for drugs, protein, glucose, and blood.
The EKG is a resting 12-lead. It’s over in five minutes. They’re screening for arrhythmias, conduction abnormalities, and early repolarization patterns. The dental exam runs quick — a visual inspection flagging anything that could become a problem at altitude, including impacted wisdom teeth and untreated decay.
The full body physical covers blood pressure, resting heart rate, height and weight against branch-specific standards, range of motion in your neck and back, and a neurological screening. The flight surgeon also reviews your complete medical history — and this is where honest disclosure matters enormously. More on that when we get to waivers.
Class I vs. Class II vs. Class III — What the Distinctions Mean
These aren’t arbitrary labels. Class I is for student pilots and initial pilot training candidates — the strictest standards, because the military is deciding whether to invest in you. Class II covers rated pilots already in the system, with slightly relaxed standards in a handful of categories. Class III applies to non-pilot aircrew — flight surgeons, combat systems officers, and similar roles. If you’re going through pilot selection, you need Class I. The standards for corrected vision, blood pressure thresholds, and waiverable conditions all shift between classes, so knowing which one applies to you before you walk in the door saves real confusion.
How to Prepare — Week Before and Day Of
Probably should have opened with this section, honestly. Preparation is where most people either help or hurt themselves — and the rules aren’t complicated, just specific.
The Week Before
Remove your contact lenses 24 hours before the exam if you wear soft lenses. Rigid gas-permeable or hard contacts require 72 hours — three full days. This is not optional and not a formality. Contacts alter the shape of your cornea, and those changes can persist well after removal. If your corneal topography looks abnormal during the ophthalmology exam, it raises immediate questions about refractive surgery history, keratoconus, and other conditions that can disqualify you outright. Bring your prescription eyeglasses. A current pair — not the ones from 2019 that you figure are probably close enough.
Skip any new supplements, mega-dose vitamins, or over-the-counter medications the week before — anything that could nudge your labs or EKG in a weird direction. No creatine loading. Creatine artificially elevates creatinine levels and can flag a kidney function concern on your metabolic panel that has no business being there. Also — apparently this needs to be said — avoid chemical relaxers or hair dyes within a few days of the exam. Some applicants have had mild allergic reactions timed just badly enough to complicate things.
Get your medical records together. All of them — surgical records, hospitalization summaries, specialist notes for anything you’ve ever been evaluated for. Treated for asthma as a kid and it resolved? Bring documentation. Took Adderall for ADHD in high school and stopped? Bring documentation of that too. The flight surgeon cannot advocate for you without paperwork. Period.
Sleep. Genuinely sleep. Blood pressure runs measurably high after poor rest, and a reading of 138/88 after five hours of anxious sleep is a problem that didn’t need to exist.
Day of the Exam
No caffeine, no nicotine, no alcohol after 2200 the night before. That’s the standard guidance — and it’s there for good reason. Nicotine elevates heart rate and blood pressure. Caffeine does the same. A single energy drink the morning of an exam has caused legitimate blood pressure spikes requiring a recheck. Just don’t.
Wear easy-to-remove clothing. You’ll be changing into a gown for parts of the exam, and elaborate lacing, compression layers, or multiple belts just slow things down and irritate the technicians. Athletic pants, a plain t-shirt, slip-on shoes. That’s all you need.
Drink water. Your veins are easier to draw from, your urine sample comes back cleaner, and you’ll feel considerably better through a long and repetitive day. A 16-ounce bottle of plain water in the waiting room is fine — just not after you’ve been told the blood draw is next.
Bring photo ID and your orders or appointment letter. Bring the name and contact information for your personal physician and any specialists you’ve seen. You may not need it — but you’ll look prepared when the flight surgeon starts asking questions, and that impression matters more than most applicants realize.
Common Disqualifiers and Waivers
Here’s the honest version of this section. Not every disqualifier ends your aviation career, but some do — and you should know the difference before you’re sitting across from a flight surgeon.
Vision
Corrected vision of 20/20 in each eye is generally acceptable across branches, even with significant refractive error, though the uncorrected standard varies considerably. LASIK and PRK are now accepted by all branches under specific conditions — the surgery must be stable for a defined period, typically 12 months, and post-op corneal thickness and refractive stability must meet branch-specific criteria. Color vision deficiency is more nuanced. Failing the PIP plates is not automatically disqualifying if you pass the FALANT or CCT. Some aviation roles still require normal color vision by strict standards, though — ask specifically about the alternative testing pathway before you assume you’re done.
Medical History
A history of migraines, diagnosed asthma, or ADHD will each get scrutinized closely. Migraines are waiverable in many cases — if they’ve been infrequent, are well-documented, haven’t required daily preventive medication in recent years, and you can show a clean window of time. Childhood asthma that resolved completely with no treatment as an adult is often waiverable. Adult-onset asthma requiring current medication is a harder case. ADHD might be the best example of the process’s complexity, as aviation medicine requires a thorough longitudinal review. That is because a prior diagnosis alone doesn’t disqualify you — but stimulant medication history, the nature of the original diagnosis, and documented functional history all factor into the decision.
The Waiver Process
Waivers exist because the military recognizes that blanket disqualifiers occasionally eliminate genuinely qualified people. But the timeline is not fast. A straightforward waiver submission to the Aeromedical Waiver Authority can take six weeks to three months. Complex cases involving specialist review, additional testing, or appeals can stretch to six months or longer.
Frustrated by the wait, many applicants make the mistake of calling the waiver authority repeatedly — a manila folder full of phone records and a reputation for being difficult to work with. That doesn’t accelerate anything. Submit complete documentation, get confirmation of receipt, and wait. What cannot be waived varies by branch but generally includes active psychosis, insulin-dependent diabetes, history of certain cancers, and severe neurological conditions. The waiver guide published by each branch’s Aeromedical Waiver Authority is the authoritative source here — not forum posts, not Reddit threads.
Branch-by-Branch Differences
The branches share a common foundation but diverge on specific standards and processing procedures. Knowing your branch’s particulars before you show up saves real time and prevents real confusion.
Air Force — Class I for UPT
The Air Force processes initial pilot training candidates through the Air Force Personnel Center (AFPC) and the Aerospace Medicine Consultation Service at Wright-Patterson AFB, Ohio. The MEPS physical is separate from the flight physical — you need both. Air Force Class I standards for uncorrected vision have loosened in recent years; the current standard allows up to -8.00 diopters of myopia for rated pilots flying with glasses or contacts, though specific programs may still carry tighter limitations. The AF uses the Aeromedical Information Management Waiver Tracking System (AIMWTS) — publicly available summaries of historically waived conditions are worth reading before you start worrying about your own history.
Army Aviation Medical Standards
Army aviation physicals are governed by Army Regulation 40-501. Class 1A is for initial selection into Army aviation. The Army has historically maintained stricter uncorrected vision standards than other branches — those standards have been revised multiple times, so verify the current version rather than relying on what someone told you two years ago. Army flight physicals are conducted at installation medical facilities by flight surgeons on the Aviation Medicine track. Processing typically runs through the Aeromedical Activity at Fort Novosel, formerly Fort Rucker, and that facility is the gating point for initial qualification.
Navy and Marine Corps Flight Physicals
Naval Aviation Medicine follows NAVMED P-117, the Manual of the Medical Department. The Naval Aerospace Medical Institute (NAMI) in Pensacola, Florida handles initial aviation candidate physicals — if you’re going through Naval Aviation Training, you will almost certainly spend time in Pensacola. That’s what makes NAMI endearing to naval aviators in a complicated way — nearly everyone who went through the pipeline has a NAMI story.
Navy flight physicals are generally considered the most thorough on the ophthalmology side. The NAMI workup for student naval aviators includes color vision testing, full ophthalmologic exam with topography, anthropometric measurements — cockpit fit is a genuine concern, you need to fit within the ejection envelope of the aircraft you’ll fly — and swim qualification and water survival screening that run separate from the medical physical itself. Processing timelines at NAMI historically run four to eight weeks for a standard case. Marine Corps aviation candidates go through the same NAMI process.
How Long Does Processing Take Overall
Realistically — and this is the number most people don’t want to hear — plan for six weeks minimum if everything in your package is clean and complete. Plan for three to six months if anything in your history requires waiver consideration. The single biggest source of delay is incomplete documentation: missing records, unsigned forms, specialist reports that weren’t included in the initial submission.
First, you should build a complete document checklist before you submit anything — at least if you want to avoid sitting in limbo wondering whether your package is even being reviewed. Ask your recruiting office or flight surgeon’s office for that checklist explicitly, then confirm every item is physically included before it leaves your hands. While you won’t need a lawyer or a medical advocate for a routine physical, you will need a handful of organized records, a clear understanding of your own medical history, and enough patience to let the process run its course. That combination — preparation, honesty, and patience — is the actual differentiator. The physical either clears you or it doesn’t, but showing up rested, documented, and ready to answer questions straight gives you the best possible version of whatever outcome the standards allow.


Leave a Reply